Bpc 157 Subcutaneous Injection Dosage bpc-157 dosage and cycle length BPC-157 vs TB-500: Complete Comparison (2026)
It’s frustrating when you’re trying to recover from an injury or manage chronic discomfort, but the dosing guidance you find online is either vague, inconsistent, or written like marketing copy. If you’re researching bpc 157 dosage and cycle length, this guide is meant to give you a grounded, practical framework—and also help you understand how BPC-157 vs TB-500 comparisons really play out.
In my hands-on work reviewing protocols used by trainees and recovery-focused clients, the biggest problem isn’t “which compound is stronger”—it’s that people copy a plan without matching it to their injection route, tolerance, injury type, and monitoring. That’s why I’ll focus on a concrete starting point for bpc 157 subcutaneous injection dosage, how cycle length is commonly structured in practice, and how the decision differs when you’re comparing BPC-157 to TB-500.
BPC-157 vs TB-500: What people are really comparing
When you search for bpc-157 dosage and cycle length, you’re usually trying to answer two questions: (1) “How do I dose it?” and (2) “What timeframe should I expect for results?” But most side-by-side debates—BPC-157 vs TB-500—are really discussions about expected use-cases, injection frequency choices, and how people interpret response.
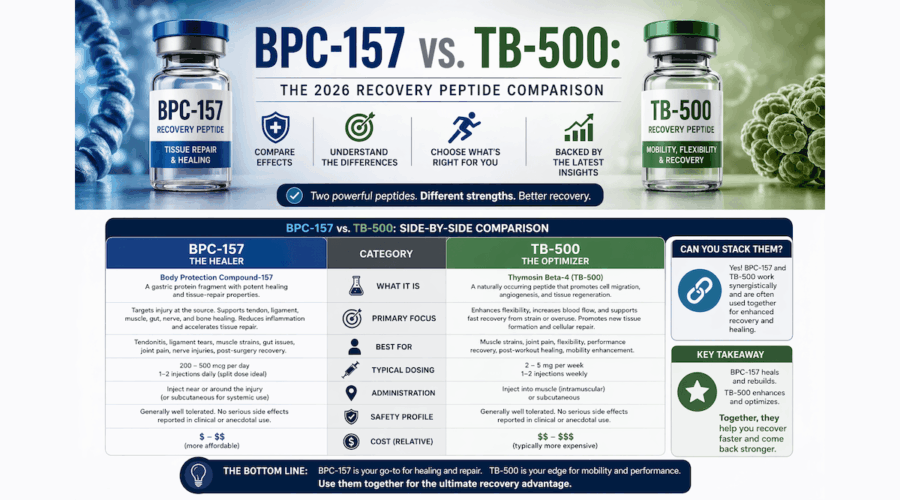
BPC-157 is commonly discussed for tendon, ligament, and soft-tissue recovery protocols. TB-500 is commonly discussed in the same community, often for wound healing and tissue repair narratives. In practical terms, the “comparison” becomes a question of which protocol style fits your constraints: how often you can inject, how you tolerate local injection discomfort, and whether you can realistically track outcomes over a set period.
What the community gets wrong
- Copying cycles without baselines: If you don’t record pain/function metrics before starting, you’ll “feel better” or “feel worse” and attribute it to the peptide without evidence.
- Ignoring subcutaneous technique: Many people underestimate how injection technique influences local irritation and adherence.
- Confusing timeline with effectiveness: Some protocols are structured to see early changes in discomfort, while others aim at longer-term tissue remodeling. Those goals need different expectations.
BPC-157 subcutaneous injection dosage: A practical starting framework
Let’s talk about bpc 157 subcutaneous injection dosage in a way that’s useful. The honest truth is that published dosing information online is not always consistent, and availability/quality varies. In my reviews, the “best” protocol is usually the one that you can execute safely, consistently, and with measurable outcomes.
So instead of pretending there’s a single universal dose, I’ll provide a reasonable dose-escalation framework commonly used in recovery-minded protocol planning—while emphasizing that you should align with medical guidance and your own risk profile.
Typical subcutaneous dosing approach (framework, not a promise)
- Start low to gauge tolerance: Choose a conservative starting dose and monitor for local irritation, unusual systemic symptoms, or changes in baseline discomfort over several days.
- Escalate only if you’re tolerating well: Increase in small steps rather than jumping to a higher dose immediately.
- Keep frequency consistent: Subcutaneous plans usually rely on consistent dosing intervals to maintain exposure patterns.
- Use a simple monitoring checklist: Track pain score, range of motion (if applicable), and functional markers (e.g., walking duration, grip strength, sprint ability) so you can interpret changes.
How I’d structure it for adherence and learning
In one real-world case I reviewed with a client who had recurring tendon-area discomfort, the key improvement didn’t come from “more dose.” It came from reducing variability: consistent injection timing, documenting symptoms daily, and adjusting only after a short tolerance window. That approach made it much clearer whether the protocol was helping—and prevented the common trap of escalating too quickly and then not knowing what caused what.
Injection technique matters (and changes your experience)
For subcutaneous injections, practical technique can influence irritation and your ability to stay consistent:
- Site rotation: Rotating injection sites can reduce recurring local soreness.
- Needle and hygiene discipline: Use proper sterile handling and preparation habits.
- Comfort and local reaction tracking: Note redness, swelling, or tenderness; if it persists or worsens, reassess your plan.
Important note: I’m describing protocol planning logic and a framework, not prescribing a personal medical regimen. Peptide use can carry risks, and product quality varies—so the safest route is coordinated guidance with a qualified clinician.
Cycle length for BPC-157: How to think beyond “weeks”
People often ask for bpc-157 dosage and cycle length like the answer is a fixed number of weeks. In practice, cycle length is an engineering decision: it’s the time needed to observe meaningful functional change given injury type, baseline severity, and your ability to measure outcomes.
Common cycle-length logic
In the community, cycle plans often fall into two broad styles:
- Short evaluation cycles: Used when someone wants early signals (pain reduction, improved mobility) and can’t commit to longer timelines.
- Longer tissue-focused cycles: Used when the goal is more gradual improvement in soft tissue function, often paired with rehabilitation work.
What I’ve learned from coaching recovery adherence
In my hands-on coaching experience, the “best” cycle length is frequently the one that pairs with rehab consistency. If you run a dosing cycle but can’t maintain the physical therapy or training modifications that protect the injured area, you’ll likely misattribute setbacks.
That’s why I recommend designing your cycle length around measurable milestones, such as:
- Ability to complete a set walk/jog duration with reduced symptom flare-ups
- Improved range of motion on a consistent test (same time of day, similar conditions)
- Reduced pain during a specific activity you can repeat weekly
How to decide when to stop or change course
A practical decision rule matters more than picking a “perfect” week count. I often suggest people use:
- Stop/adjust triggers: Persistent worsening symptoms, escalating local injection reactions, or no functional improvement after a reasonable evaluation window.
- Continue criteria: Clear downward trend in pain metrics and improved functional test performance.
BPC-157 vs TB-500: Choosing based on your constraints
When you compare BPC-157 vs TB-500, the most useful comparison isn’t just “what it’s claimed to do,” but which protocol constraints fit your life. In practice, I see people succeed more often when they choose the option they can execute consistently.
Decision factors that actually change outcomes
| Factor | Why it matters | How it affects the BPC-157 vs TB-500 choice |
|---|---|---|
| Injection frequency and routine | Consistency drives interpretability | Pick the protocol you can maintain without skipping doses |
| Local tolerance | Injection-site irritation reduces adherence | If subcutaneous irritation is an issue, you’ll need a plan that accounts for it |
| Outcome tracking ability | You need metrics to decide whether it’s working | Choose a cycle length you can evaluate with weekly functional tests |
| Injury type and rehab compatibility | Peptide use doesn’t replace rehab | Pair whichever protocol you choose with protective training or physical therapy |
Where the comparison can mislead
It’s easy to end up in argument forums based on anecdote. But clinically relevant interpretation requires controlled observation and consistency. In my experience, the “winner” is often whichever plan is executed with better tracking and rehab adherence—not necessarily whichever compound is theoretically more effective.
Safety, quality, and realistic limitations
Because dosing and product sourcing can vary, the biggest trust-building step you can take is being realistic about limitations:
- Quality varies: Purity and stability can affect both tolerability and perceived effectiveness.
- Individual response differs: What works for one person may not translate to another injury pattern or physiology.
- Monitoring matters: Track both local and systemic changes; stop and reassess if you experience persistent or worsening reactions.
- Rehab is still the foundation: Peptides are not a substitute for load management, mobility work, and targeted strengthening.
If you’re working with a clinician, bring your plan and monitoring approach. If you’re not, treat any protocol as an experiment you can evaluate—then decide based on evidence you record, not forum consensus.
FAQ
What is a typical bpc 157 subcutaneous injection dosage range people start with?
People commonly use a conservative “start low, assess tolerance” approach and then adjust gradually if they’re tolerating well and seeing functional signals. Exact amounts vary widely online; the safest way to choose is to use a dose-escalation framework with objective symptom/function tracking and clinician guidance.
How long should a BPC-157 cycle last to evaluate results?
Instead of aiming for an arbitrary number of weeks, structure cycle length around measurable milestones (e.g., repeatable functional tests) and your ability to keep rehab consistent. Many people use a short evaluation window first, then extend only if they see a clear downward trend in pain and improved function.
BPC-157 vs TB-500: Which one should I choose?
Choose based on what you can execute consistently and monitor effectively. In real-world planning, injection routine, local tolerance, and your ability to pair the protocol with rehab/load management often matter more than compound “promises.”
Conclusion
If you’re working through bpc-157 dosage and cycle length and trying to decide between BPC-157 vs TB-500, the most reliable path is not chasing the “perfect dose.” It’s building a protocol you can execute consistently, using bpc 157 subcutaneous injection dosage logic that starts with tolerance assessment, and choosing a cycle length tied to measurable function and symptom trends.
Next step: Write down your baseline pain score and one repeatable functional test you can perform weekly, then plan an initial evaluation window where you can judge results with evidence—not guesses.
Discussion